Calculate Q angle from ASIS and tibial-tuberosity landmark offsets, then compare the result with common adult reference bands.
Last updated
Q angle measurement workflow Enter landmark offsets from the patella centre, keep every measurement in the same unit, and compare repeated readings only when the stance and landmark method are the same.
Quick examples
Measurement unit
Reference band
Use the same unit for every offset. The angle stays the same whether you measure in millimetres, centimetres, or inches.
Enter all four landmark offsets Add the ASIS and tibial-tuberosity offsets from the patella centre in one consistent unit to calculate the Q angle and compare it with common adult reference bands.
Q angle calculator guide: measuring quadriceps angle from knee landmarks
A Q angle calculator estimates the angle between the quadriceps line of pull and the patellar tendon line. This page uses frontal-plane landmark offsets from the patella centre to estimate the angle, then compares it with common adult reference bands while keeping clear non-diagnostic framing.
What the Q angle is measuring
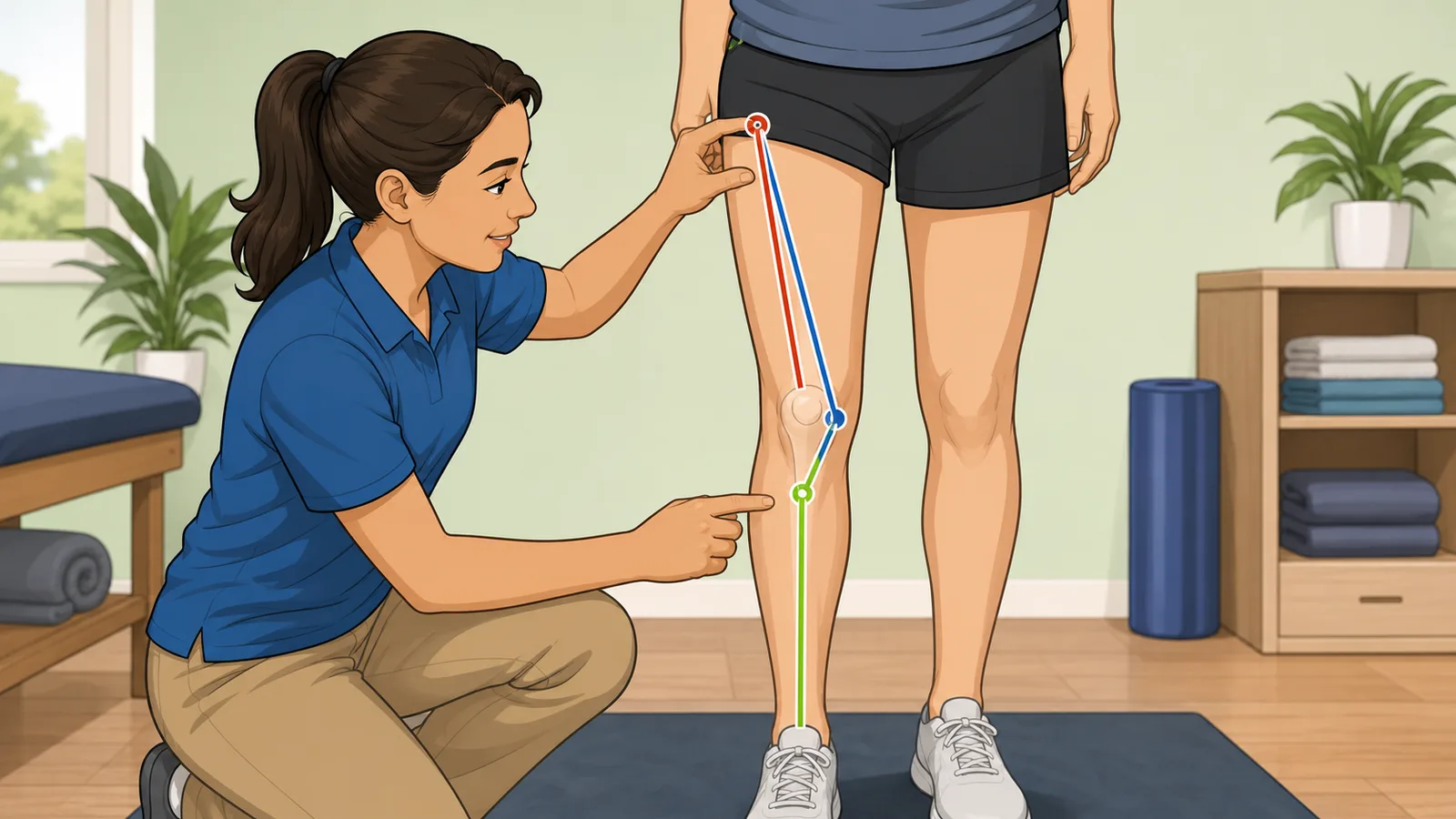
The quadriceps angle, usually shortened to Q angle, describes the angle formed by the line from the anterior superior iliac spine (ASIS) to the patella and the line from the patella to the tibial tuberosity. Clinicians and sports-medicine texts use it as one way to describe frontal-plane alignment around the knee and patellofemoral mechanism.
That matters because the angle is sometimes discussed when clinicians assess anterior knee pain, patellar tracking, or lower-limb alignment. But the Q angle should not be treated as a stand-alone diagnosis. Symptoms, movement quality, training load, and other physical-exam findings can matter more than the number itself.
How this calculator turns landmark offsets into a Q angle
This page assumes the patella centre is the reference point. You enter how far laterally and vertically the ASIS sits from that point, and how far laterally and vertically the tibial tuberosity sits from it. Because the calculation is geometric, the actual unit does not matter as long as every offset uses the same unit.
The calculator then forms the ASIS-to-patella vector and the patella-to-tibial-tuberosity vector and computes the included angle between them. That provides a reproducible estimate from a consistent landmark method without forcing you to measure two separate line angles by hand.
Q angle = arccos((u · v) ÷ (|u| × |v|))
u is the ASIS-to-patella vector and v is the patella-to-tibial-tuberosity vector.
Reference ranges are only rough screening bands
Many texts quote rough adult reference values around 10° to 15° for men and about 15° to 20° for women, but published studies show substantial measurement variability. Landmark placement, standing versus supine position, limb rotation, and examiner technique can all change the reported angle.
That means the comparison rows on this page are best used as orientation, not as a pass-fail judgement. A higher or lower angle can be worth discussing in context when someone has knee symptoms, but a normal-looking angle does not rule problems out and a higher angle does not prove patellofemoral pathology on its own.
Why measurement position and landmark consistency matter
A Q angle taken standing is not always directly interchangeable with one taken supine, and a value measured with the quadriceps relaxed is not always comparable with one taken during an active contraction. That is one reason strong Q-angle interpretation focuses on repeatable technique before it focuses on tiny degree differences.
If you are using this page to track change over time, keep the same posture, foot position, limb rotation, and landmark method every time. The most useful comparison is usually not your result against a universal perfect number. It is your result against a prior measure collected the same way.
Worked example: estimating a Q angle from four offsets
Suppose the ASIS sits 1.5 cm lateral and 12 cm superior to the patella centre, while the tibial tuberosity sits 1 cm lateral and 6 cm inferior to the patella centre. Using those offsets, the calculator estimates a Q angle of about 16.6°.
With the female reference band selected, that lands inside the common adult reference range. With the male reference band selected, the same geometry falls above the usual quoted range. That difference is why the comparison band should always be read as context rather than as a diagnosis.
Why the unit does not change the angle
The calculator uses geometry rather than an absolute-distance threshold. Because both landmark lines scale together, the Q angle stays the same whether you enter the offsets in millimetres, centimetres, or inches, as long as every value uses the same unit.
That makes the tool flexible in clinic and sport settings where one assessor may work in centimetres and another may work in millimetres. The important part is consistency inside the same measurement, not the specific unit system itself.
When a Q angle should not be used alone
Q-angle measurement can be unreliable when landmark placement is inconsistent or when the person changes stance, hip rotation, or knee position between readings. Repeated measures are most useful when the same clinician and same landmark method are used each time.
If someone has significant knee pain, recurrent patellar instability, swelling, trauma, or functional limitation, a clinician should assess the full picture instead of relying on a single alignment angle. The page is best used as an educational screening aid and communication tool, not as a replacement for a musculoskeletal exam.
Frequently asked questions
What is a normal Q angle?
Common adult reference values are often quoted as roughly 10° to 15° for men and about 15° to 20° for women, but those bands vary across studies and measurement methods. They are best treated as rough screening ranges rather than strict cutoffs.
Can a high Q angle diagnose patellofemoral pain?
No. A higher Q angle can appear in people with anterior knee pain, but it does not diagnose patellofemoral pain syndrome or patellar instability by itself. Symptoms, movement assessment, strength, training load, and other exam findings still matter.
Does it matter whether I measure in centimetres or millimetres?
No, as long as every offset uses the same unit. The calculator is based on geometry, so the angle stays the same whether the landmark distances are entered in centimetres, millimetres, or inches.
Why can two clinicians get different Q-angle values?
Because the measurement is sensitive to landmark placement, limb rotation, stance, and whether the person is assessed standing or supine. That is one reason Q angle has limited reliability when it is used casually or without a standardised protocol.
How do I measure Q angle more consistently?
Use the same posture, the same patella-centre reference, the same limb rotation, and the same ASIS and tibial-tuberosity landmark method each time. Repeatability matters more than chasing a single perfect landmark setup once.
Does standing versus supine position change Q angle?
It can. Published studies show that posture and lower-limb position can shift the measured angle, which is why repeated readings are most useful when the same protocol is used each time.
Can I enter the offsets in inches instead of centimetres?
Yes. The angle is scale-independent, so inches, centimetres, or millimetres all work as long as every offset in the same calculation uses the same unit.